Abstract
Background: Adverse event reporting is a fundamental component of patient safety and healthcare quality improvement; however, underreporting remains a persistent challenge, particularly in low- and middle-income countries. Behavioral, cultural, and system-level barriers often limit the effectiveness of adverse event reporting systems. Objective: To evaluate the effectiveness of a structured quality improvement intervention in enhancing adverse event reporting in a secondary care hospital in Sri Lanka. Methods: A mixed-methods quality improvement study was conducted at Base Hospital Kalmunai North, Sri Lanka, from January to December 2025. The DMAIC (Define–Measure–Analyze–Improve–Control) framework guided the intervention. Baseline adverse event reporting trends were assessed retrospectively, while barriers and facilitators to reporting were explored through focus group discussions. Interventions were designed using the COM-B (Capability, Opportunity, Motivation–Behaviour) model to address identified behavioral determinants. Reporting trends before and after the intervention were compared using descriptive statistics. Results: Following implementation of the intervention, adverse event reporting increased to 61 reports in 2025, compared with 43 reports in 2023 and 37 reports in 2024, representing a 60.7% increase compared with 2024. Reporting patterns became more consistent and sustained throughout the year. In addition to increased reporting frequency, new categories of adverse events, including wrong drug dose administration and missed drug doses, were reported, suggesting improved staff awareness, engagement, and willingness to report medication-related incidents beyond previously recognized categories. Conclusion: A structured, DMAIC-guided, behaviorally informed intervention incorporating the COM-B model significantly improved adverse event reporting in a secondary care hospital. This practical, low-cost, and scalable approach demonstrates the potential to strengthen patient safety culture and adverse event reporting systems in resource-limited healthcare settings.
Keywords
Adverse event reporting Patient safety Quality improvement DMAIC COM-B Just culture Sri Lanka.
1. Introduction
Adverse events are a major challenge to patient safety worldwide, referring to harm arising from healthcare delivery rather than the patient’s underlying condition. The WHO defines an adverse event as any unintended medical occurrence temporally associated with a medicinal product or device, while the NIH describes them as injuries or complications from medical management, including medication errors, procedural complications, healthcare-associated infections, psychological harm, and death (1,10,12).
In Sri Lanka, the Directorate of Healthcare Quality and Patient Safety (DHQS) defines adverse events as injuries related to medical management, encompassing all aspects of care such as diagnosis, treatment, and system or equipment use. Events may be preventable or non-preventable, and systematic identification is crucial for patient safety and healthcare quality improvement (13).
The DHQS guidelines emphasize non-punitive reporting, constructive organizational responses, trained personnel, and adequate resources. Reporting enables risk identification, detection of system failures, early warning of hazards, and organizational learning (4,6,13). Recent initiatives, such as QR code–based reporting of adverse drug reactions to the NMRA, support these efforts. Yet underreporting remains widespread due to fear of blame, lack of awareness, complex processes, workload, and limited feedback (4,6,7,9).
Globally, adverse events are common in both low- and high-income countries, highlighting the need for effective reporting systems (2,3). In Sri Lanka, hospital reporting often focuses on non-clinical events, with significant underreporting of clinically relevant incidents (8).
This study evaluated a structured, multimodal intervention at a secondary care hospital, using the DMAIC (Define, Measure, Analyze, Improve, Control) framework and the COM-B (Capability, Opportunity, Motivation–Behaviour) model. By integrating quantitative trends with qualitative staff perspectives, the study explores both the intervention’s effectiveness and the behavioral drivers of improved reporting.
2. Literature Review
Adverse event reporting is widely recognized as a cornerstone of patient safety, providing critical insights into system vulnerabilities and opportunities for organizational learning. However, despite its importance, underreporting of adverse events remains a persistent challenge across healthcare settings globally.
Several studies have consistently identified practical and behavioral barriers to adverse event reporting. Tevis, Schmocker, and Wetterneck demonstrated that among medical residents, lack of knowledge on how to submit reports and insufficient time were key deterrents to reporting. Importantly, their study showed that targeted education combined with simplification of the reporting process resulted in a 230% increase in annual adverse event reports (from 68 to 154 reports; p = 0.025), highlighting the effectiveness of addressing both capability and opportunity-related barriers (1).
At a systems level, a systematic review focusing on emergency departments found that unified reporting systems, technology-based solutions, and collaborative models of care were central to both reducing adverse events and improving reporting practices. These findings reinforce the need for structured, user-friendly systems that support frontline healthcare workers in reporting safety incidents without undue burden (3).
Beyond structural barriers, organizational culture plays a pivotal role in shaping reporting behavior. Kumah emphasized that adverse events—defined as unintended injuries or complications resulting from healthcare management—offer valuable insights into systemic weaknesses. However, fear of punitive action, reputational damage, and legal repercussions frequently discourage reporting. To address this, the author stresses the adoption of a just culture, supported by standardized frameworks for evaluating errors, leadership commitment, psychological safety, and balanced accountability. Learning from errors, rather than assigning blame, is identified as essential for sustainable safety improvement (4).
The concept of just culture has been widely discussed across healthcare and other high-risk industries. Heraghty et al. describe just culture as an organizational approach aimed at achieving fair outcomes for individuals involved in adverse events or near misses (7). Such approaches prioritize transparency, trust, and continuous improvement over fear and silence. However, cultivating a strong safety culture is complex and requires sustained effort, with no guaranteed success (6). Leadership support, structured reporting and analysis processes, and a commitment to ethical accountability are critical enablers. Open communication, including space to discuss incidents and emotional responses, is perceived as essential, though challenges remain in balancing openness with individual responsibility and procedural consequences (6,7).
Evidence from Sri Lanka reflects similar patterns. Mallawarachchi and Dharmarathna, in their assessment of adverse event reporting in selected state hospitals, found that most reported events were non-clinical, particularly patient falls (30.46%) (8). Strengths of the system included the availability of national guidelines, established quality management units, and a non-punitive approach to reporting and analysis. However, lengthy paper-based documentation was identified as a major weakness, limiting broader engagement and timely reporting. The study concluded that while an adverse event reporting framework exists in Sri Lanka, its utilization remains narrow and suboptimal (8).
Further supporting these findings, Majda et al. reported that excessively complex paperwork, perception of minimal patient harm, and fear of negative consequences were the most common reasons for abandoning adverse event reporting among nurses and midwives (9). Creating a supportive environment where staff can report errors honestly and without fear was identified as a key strategy for improvement. Phillips et al. similarly emphasized the importance of training healthcare professionals in interpersonal communication skills and fostering an open organizational culture where adverse event communication and disclosure are normalized practices (10). Earlier work by Leape highlighted that reporting systems are most effective when they are confidential, easy to use, provide expert analysis, and offer timely feedback—conditions that remain unmet in many settings (12).
In response to these recognized challenges, the Directorate of Healthcare Quality and Patient Safety (DHQS) of the Ministry of Health, Sri Lanka, introduced national Adverse Event Reporting Guidelines in 2016 (13). These guidelines aim to strengthen reporting systems by focusing on system failures rather than individual blame. The reporting mechanism is structured into two components: Part A, which can be completed by any healthcare worker in their own language within 24 hours of the event, and Part B, which is completed by the head of the unit and focuses on root cause analysis, contributing factors, and preventive measures following team discussion (Annexure I) (13). While this framework provides a strong foundation, effective implementation depends on staff capability, motivation, and organizational support.
3. Objective
to evaluate the effectiveness of a structured intervention on improving adverse event reporting at a secondary care hospital in Sri Lanka.
4. Methodology
4.1Study Design and Setting
This study employed a mixed-methods quality improvement design conducted at Base Hospital Kalmunai North (BHKN), a Type A secondary care hospital located in the Eastern Province of Sri Lanka with bed strength of 413. The hospital provides services to a diverse patient population and is staffed by a multidisciplinary healthcare workforce.
The study was conducted over a 12-month period from January to December 2025 and included baseline assessment, intervention implementation, and post-intervention evaluation. The DMAIC (Define–Measure–Analyze–Improve–Control) framework was used to guide systematic problem identification, data-driven analysis, implementation of targeted interventions, and sustainability planning.
4.1.1 Define Phase
A preliminary review of adverse event reporting trends at BHKN was conducted using records maintained by the Quality Management Unit (QMU). This review identified a decline in reporting, with 43 adverse events reported in 2023 compared with 37 events in 2024.
During the third-quarter Quality Steering Committee meeting in 2024, the importance of adverse event reporting in strengthening patient safety culture was emphasized, and a structured quality improvement project was initiated to enhance adverse event reporting across the hospital.
4.1.2 Measure Phase
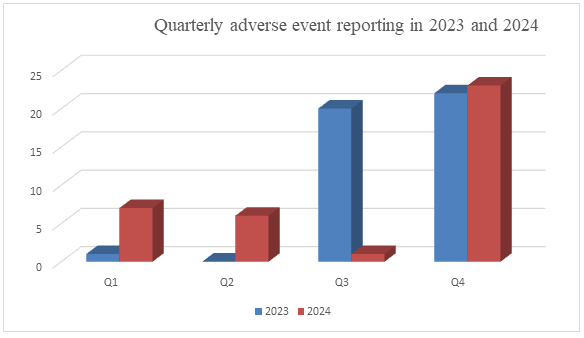
Baseline measurement was conducted using adverse event reports submitted to the QMU through standardized reporting forms. Quarterly analysis of reports from 2023 and 2024 demonstrated inconsistent reporting patterns, with particularly low reporting during the first and second quarters of both years and a further decline in the third quarter of 2024.
Figure 1 illustrates the quarterly distribution of adverse event reports during 2023 and 2024.
| Year | fall | Drug Allergy | Needle prick | Blood reaction | Assault | Others | Total |
| 2023 | 13 | 6 | 8 | 7 | 2 | 9 | 43 |
| 2024 | 11 | 7 | 5 | 12 | 0 | 2 | 37 |
Table 1- categorical descriptionof adverse events reported in 2023 and 2024 at BHKN
To explore the underlying causes of under-reporting, a qualitative assessment was undertaken to identify perceived barriers and facilitators of adverse event reporting. Audio-recorded focus group discussions (FGDs) were conducted with eight nursing officers representing key clinical areas, including medical, surgical, paediatric, obstetrics and gynaecology wards, the Accident and Emergency Unit, Blood Bank, Mental Health Unit, Intensive Care Unit, and Operating Theatre.
The discussions explored:
-
Knowledge and awareness of adverse event reporting
-
Current reporting practices
-
Individual, organizational, system, and cultural barriers
-
Organizational culture and leadership influence;
-
Facilitators of reporting and Recommendations for improvement.
Audio recordings were transcribed verbatim, and thematic analysis was performed to identify key patterns and root causes of under-reporting.
4.1.3.Analyze Phase
The thematic analysis identified several interrelated factors contributing to under-reporting Participants reported fear of blame, legal consequences, interpersonal conflict, and negative professional perceptions as major deterrents. Organizational challenges included heavy workload, staffing pressures, lack of structured review mechanisms, and limited leadership engagement. System-level issues included complex, paper-based reporting forms and unclear reporting criteria. Cultural barriers reflected a prevailing blame-oriented environment rather than a learning-focused safety culture.
4.1.4.Improve Phase
Findings from the Define, Measure, and Analyze phases indicated that under-reporting was influenced by both process deficiencies and behavioral factors, including limited knowledge, fear of punitive action, time constraints, and low perceived value of reporting. To address these determinants, the COM-B (Capability, Opportunity, Motivation–Behaviour) model was integrated into the improvement phase.
Identified barriers were mapped to the COM-B domains:
-
Capability: Limited understanding of patient safety concepts, adverse event definitions, and reporting procedures.
-
Opportunity: Time constraints, heavy workload, complex reporting processes, and limited opportunities for discussion.
-
Motivation: Fear of blame and legal consequences, lack of feedback, absence of recognition, and low perceived impact of reporting.
Capability-enhancing interventions
A Training of Trainers (TOT) programme was conducted for 20 selected nursing officers to develop patient safety champions. The programme was facilitated by a qualified patient safety expert and ISQua member. Patient safety champions subsequently conducted unit-level training sessions, motivational activities, and role plays.
The TOT programme consisted of eight interactive sessions (four hours each) incorporating workshops, simulations, group discussions, and peer teaching. Training topics included patient safety fundamentals, medication safety, communication and teamwork, risk management and incident reporting, infection prevention, international patient safety goals, and bridging the knowing–doing gap. A patient safety training module was developed following programme completion.
In addition, twice-monthly training sessions (two hours per session) were conducted by the QMU for nursing officers and medical officers to improve understanding of adverse event definitions, reporting processes, non-punitive reporting principles, and the evolution of safety culture from pathological to generative stages.
Structured training programmes were also conducted for healthcare assistants, cleaning service staff, and security personnel to promote their role as safety observers and encourage initiation of adverse event reporting.
Regular review meetings involving hospital leadership and the QMU were conducted to reinforce knowledge, clarify reporting processes, and promote trust and open communication.
Opportunity-enhancing interventions
Opportunities for reporting were strengthened through unit-level adverse event presentations during monthly Quality Circle meetings, multidisciplinary discussions, and expert reviews focusing on root causes, corrective actions, adherence to standard operating procedures, and preventive strategies. The Director or Deputy Director and QMU staff actively participated in these meetings.
Additional interventions included regular reminders through WhatsApp communication platforms, safety huddles, and role-play activities emphasizing the importance of adverse event reporting. Monthly adverse event review meetings were conducted to perform root cause analyses, recognize units with higher reporting rates, implement corrective measures, provide opportunities for staff reflection, and reinforce adherence to standard protocols within a no-blame, no-shame culture.
Motivation-enhancing interventions
Motivation was strengthened through recognition of reporting units, sharing success stories, timely feedback, and demonstration of the impact of reporting on patient safety outcomes. Leadership commitment, balanced accountability, and psychological support were emphasized to reduce fear and encourage reporting.
4.1.5.Control Phase
To sustain improvements, structured review meetings were scheduled using a predefined calendar. Adverse event reporting trends were continuously monitored at unit level, and results were shared during reviews and through institutional communication channels.
Necessary resources were provided, including fall risk assessment tools, medication safety aids, and allergy identification cards. Refresher training programmes were conducted as required. All review activities were led by the Director or Deputy Director, reinforcing leadership commitment to patient safety and a non-punitive reporting culture.
5. Results
Adverse event reports submitted to the hospital reporting system were retrospectively collected for 2023 and 2024 and prospectively monitored for 12 months following implementation of the intervention in 2025. Data included both the number and categories of reported adverse events.
Descriptive statistics were used to summarize reporting trends before and after the intervention. Percentage changes in reporting rates were calculated to assess the impact of the quality improvement initiative.
Post-intervention analysis demonstrated a substantial improvement in adverse event reporting at BHKN. Figure 2 illustrates reporting trends for 2023, 2024, and 2025.
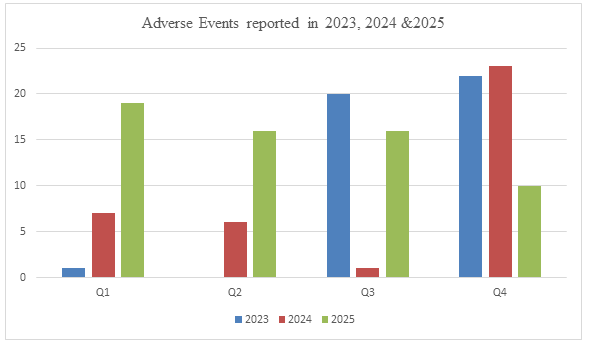
Following implementation of the structured intervention, adverse event reporting in 2025 showed a more stable and sustained pattern throughout the year compared with the fluctuating and declining trends observed in previous years. A total of 61 adverse events were reported in 2025, compared with 43 events in 2023 and 37 events in 2024. Compared with 2024, this represents a 60.65% increase in adverse event reporting.
Categorical analysis demonstrated not only an increase in reporting frequency but also improved diversity of reporting. Notably, previously unreported categories, including wrong drug dose administration and missed drug dosage, were identified in 2025, suggesting enhanced awareness and reporting practices among healthcare staff. Table 2 presents the distribution of adverse event categories reported during the study period.
| Year | fall | Drug Allergy | Needle prick | Blood reaction | assault | Wrong drug dose | Missed drug dose | Others | Total |
| 2023 | 13 | 6 | 8 | 7 | 2 | 0 | 0 | 9 | 43 |
| 2024 | 11 | 7 | 5 | 12 | 0 | 0 | 0 | 2 | 37 |
| 2025 | 17 | 6 | 7 | 14 | 8 | 1 | 2 | 4 | 61 |
6. Discussion
This study demonstrated that a structured, multimodal intervention informed by the DMAIC quality improvement framework and the COM-B behavioral model substantially improved adverse event reporting in a secondary care hospital setting.
Targeted training interventions were central to improving reporting by addressing capability gaps identified during the Analyze phase. The Training of Trainers (TOT) programme enhanced staff knowledge of patient safety principles, clarified adverse event definitions, and strengthened reporting competencies. By bridging the "knowing-doing gap," training empowered frontline staff to recognize and report incidents more effectively. Similar findings have been reported by Tevis et al., who demonstrated that educational interventions combined with simplified reporting processes significantly increased adverse event reporting rates (1).
Positive reinforcement strategies also contributed to sustained reporting behavior. Recognition of reporting units, dissemination of success stories, and constructive feedback reinforced the perception that reporting contributes to meaningful organizational improvement. Previous studies have similarly identified feedback and acknowledgment as important facilitators of reporting compliance (9,12).
The introduction of a non-punitive, just culture addressed several fear-based barriers, including concerns related to blame, legal consequences, and interpersonal conflict. Leadership-led reviews, open discussions, and balanced accountability facilitated a shift from a blame-oriented culture toward a learning-oriented patient safety culture. These findings are consistent with previous evidence demonstrating that reporting systems function most effectively within organizations that promote psychological safety, transparency, and continuous learning (4,6,7).
Studies conducted both internationally and within Sri Lanka have reported similar challenges. Tevis et al. demonstrated a 230% increase in adverse event reporting following educational and system-level interventions (1), while Mallawarachchi and Dharmarathna reported that adverse event reporting in Sri Lankan hospitals remained limited by process complexity and organizational culture (8). The present study extends these findings by demonstrating that behaviorally informed interventions, rather than structural modifications alone, can significantly improve adverse event reporting practices.
This intervention has particular relevance for resource-constrained healthcare settings because it relies primarily on leadership engagement, staff empowerment, structured communication, and existing institutional mechanisms rather than substantial financial investment. The integration of the COM-B model within the DMAIC framework provides a practical and scalable approach for strengthening patient safety culture and adverse event reporting systems.
7. Strengths and Limitations
Strengths
-
Use of a structured quality improvement framework (DMAIC) combined with a behavioral change model (COM-B)
-
Practical, low-cost intervention suitable for public sector hospitals
-
Strong leadership involvement and multidisciplinary engagement
-
Integration of both quantitative outcomes and qualitative insights
Limitations
-
Single-center study, which may limit generalizability
-
Relatively short post-intervention follow-up period
-
Potential reporting bias, as increased awareness may influence reporting behavior
8. Conclusion
This study demonstrates that a structured, multimodal intervention incorporating staff training, system strengthening, leadership engagement, and positive reinforcement significantly improved adverse event reporting at a secondary care hospital in Sri Lanka. By addressing both system-level and behavioral determinants of reporting through the DMAIC and COM-B frameworks, the intervention fostered a more open, learning-oriented patient safety culture.
9. Recommendations
-
Implement regular patient safety and adverse event reporting training for all healthcare staff
-
Strengthen institutional policy support for non-punitive, just culture-based reporting
-
Integrate adverse event reporting initiatives into hospital patient safety and quality improvement programs
-
Establish routine feedback and learning mechanisms following reported events
-
Explore progressive digitalization of reporting systems to further reduce reporting burden
Acknowledgement: Dr TSRTR Rajab MBBS, MSc, MBA, EMBA, FCAM,Member of ISQUA
References
- Tevis SE, Schmocker RK, Wetterneck TB. Adverse event reporting: harnessing residents to improve patient safety. J Patient Saf. 2020;16(4):294–298. doi: DOI ↗ Google Scholar ↗
- Kimball M, Wagenaar BH. Applying a systems lens to understand patient safety effectiveness in low- and middle-income countries. BMJ Qual Saf. 2022;31(5):e1–e9. doi: DOI ↗ Google Scholar ↗
- Afolalu OO, Akpor OA, Afolalu SA. A systematic review of interventions for reducing and reporting adverse events in emergency departments: multidisciplinary approaches and technological innovations. Collegian. 2025;32(1):34–45. doi: DOI ↗ Google Scholar ↗
- Kumah A. Adverse event reporting and patient safety: the role of a just culture. Front Health Serv. 2025;5:1581516. doi: DOI ↗ Google Scholar ↗
- Kumah A, Nwogu CN, Issah AR, et al. Cause-and-effect (fishbone) diagram: a tool for generating and organizing quality improvement ideas. Glob J Qual Saf Healthc. 2024;7(2):85–87. doi: DOI ↗ Google Scholar ↗
- van Baarle E, Hartman L, Rooijakkers S, et al. Fostering a just culture in healthcare organizations: experiences in practice. BMC Health Serv Res. 2022;22:1035. doi: DOI ↗ Google Scholar ↗
- Heraghty D, Rae AJ, Dekker SWA. Managing accidents using retributive justice mechanisms: when the just culture policy gets done to you. Saf Sci. 2020;126:104677. doi: DOI ↗ Google Scholar ↗
- Mallawarachchi S, Dharmarathna G. A systematic assessment of adverse event reporting in selected state hospitals in Sri Lanka. J Surg Med. 2022;6(4):494–497. DOI ↗ Google Scholar ↗
- Majda A, Majkut M, Wróbel A, et al. Perceptions of clinical adverse event reporting by nurses and midwives. Healthcare (Basel). 2024;12(4):460. doi: DOI ↗ Google Scholar ↗
- Phillips R, Hazell L, Sauzet O, et al. Analysis and reporting of adverse events in randomised controlled trials: a review. BMJ Open. 2019;9:e024537. doi: DOI ↗ Google Scholar ↗
- Myren BJ, de Hullu JA, Bastiaans S, et al. Disclosing adverse events in clinical practice: the delicate act of being open. Health Commun. 2022;37(2):191–201. doi: DOI ↗ Google Scholar ↗
- Leape LL. Reporting of adverse events. N Engl J Med. 2002;347(20):1633–1638. doi: DOI ↗ Google Scholar ↗
- Directorate of Healthcare Quality and Patient Safety. Adverse Event Reporting Guidelines. Ministry of Health, Sri Lanka; 2016. DOI ↗ Google Scholar ↗